Anti-Tumor Potential of a 5-HT3 Receptor Antagonist as a Novel Autophagy Inducer in Lung Cancer: A Retrospective Clinical Study with In Vitro Confirmation

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Retrospective Study
2.1.1. Study Population and Design
2.1.2. Statistical Analysis
2.2. In Vitro Study
2.2.1. Cell Cultures and Drug Treatment
2.2.2. Flow Cytometry
2.2.3. Cell Viability
2.2.4. Cell Scraping Assay
2.2.5. Clonogenic Assay
2.2.6. Western Blot Analysis
2.2.7. Autophagic Flux Assay
2.2.8. Statistical Analysis
3. Results
3.1. Study Population, Demographic Data, and Perioperative Characteristics
3.2. Association between the Use of Palonosetron or Ramosetron, Cancer Recurrence, and Mortality after Surgery
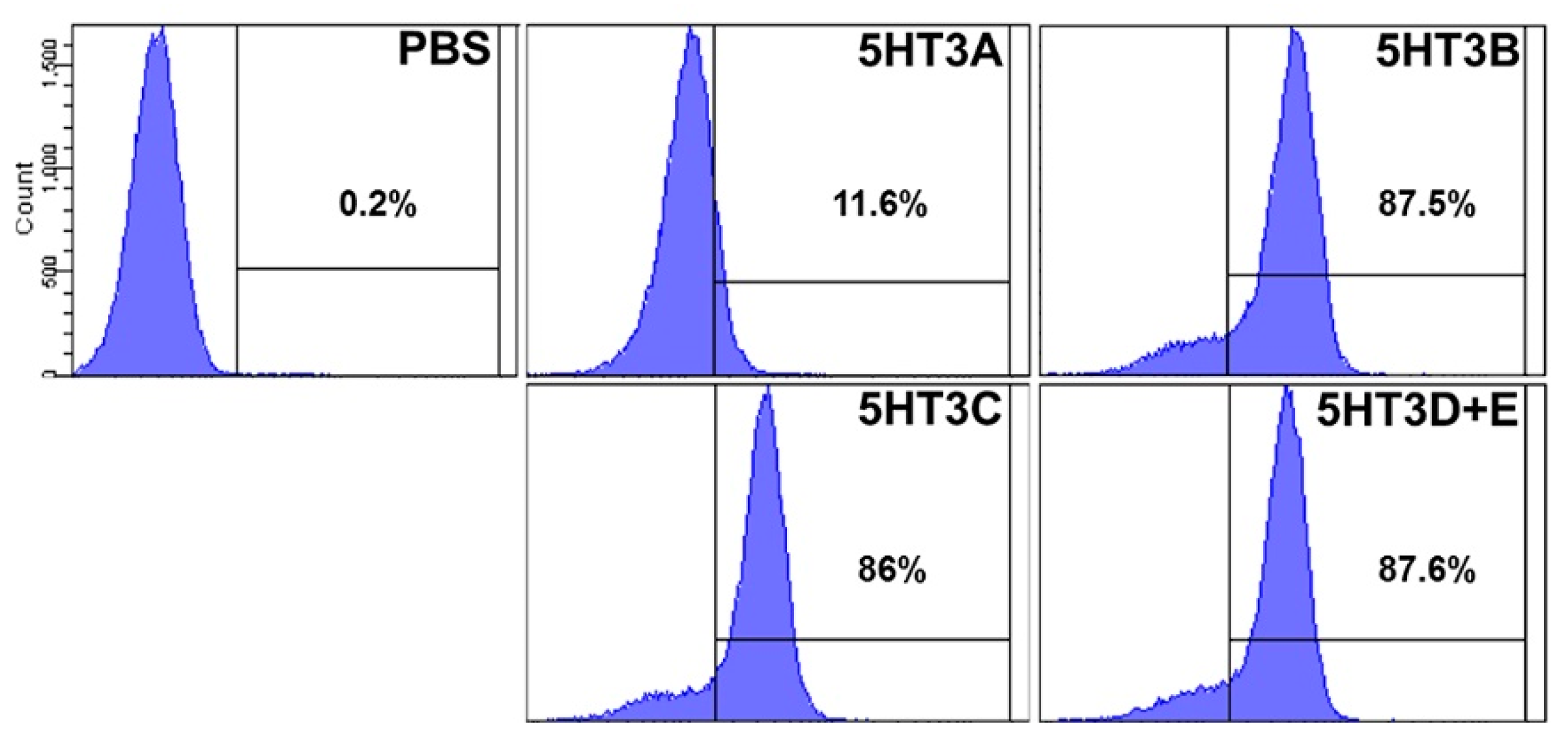
3.3. 5-HT3 Receptor Confirmation in A549 Cell
3.4. 5-HT3RAs Inhibit A549 Cell Proliferation in a Dose-Dependent Manner
3.5. 5-HT3RAs Inhibit Cell Migration and Colony Formation in A549 Cells
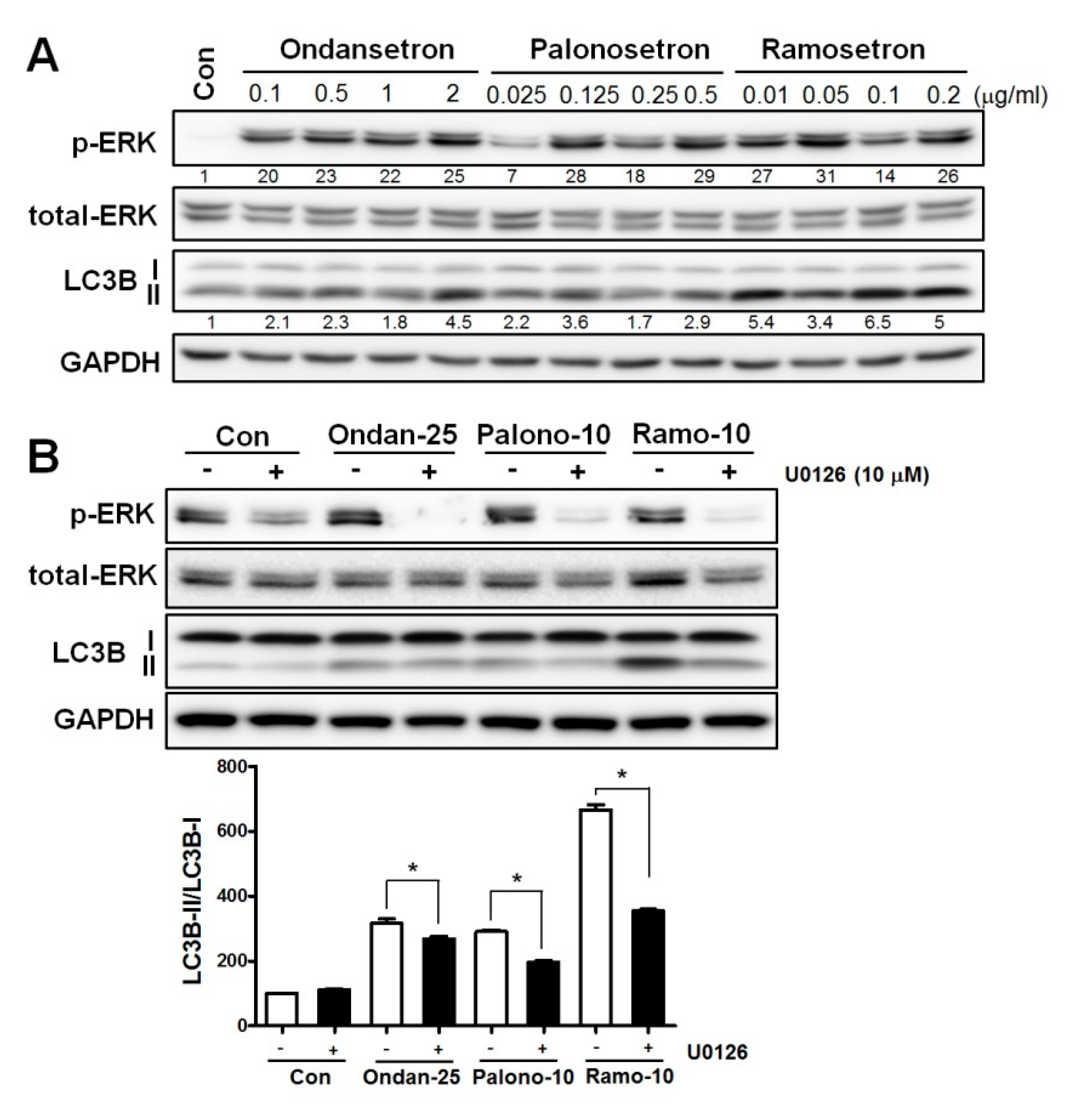
3.6. 5-HT3RAs Induce Autophagy via the ERK Signaling Pathway
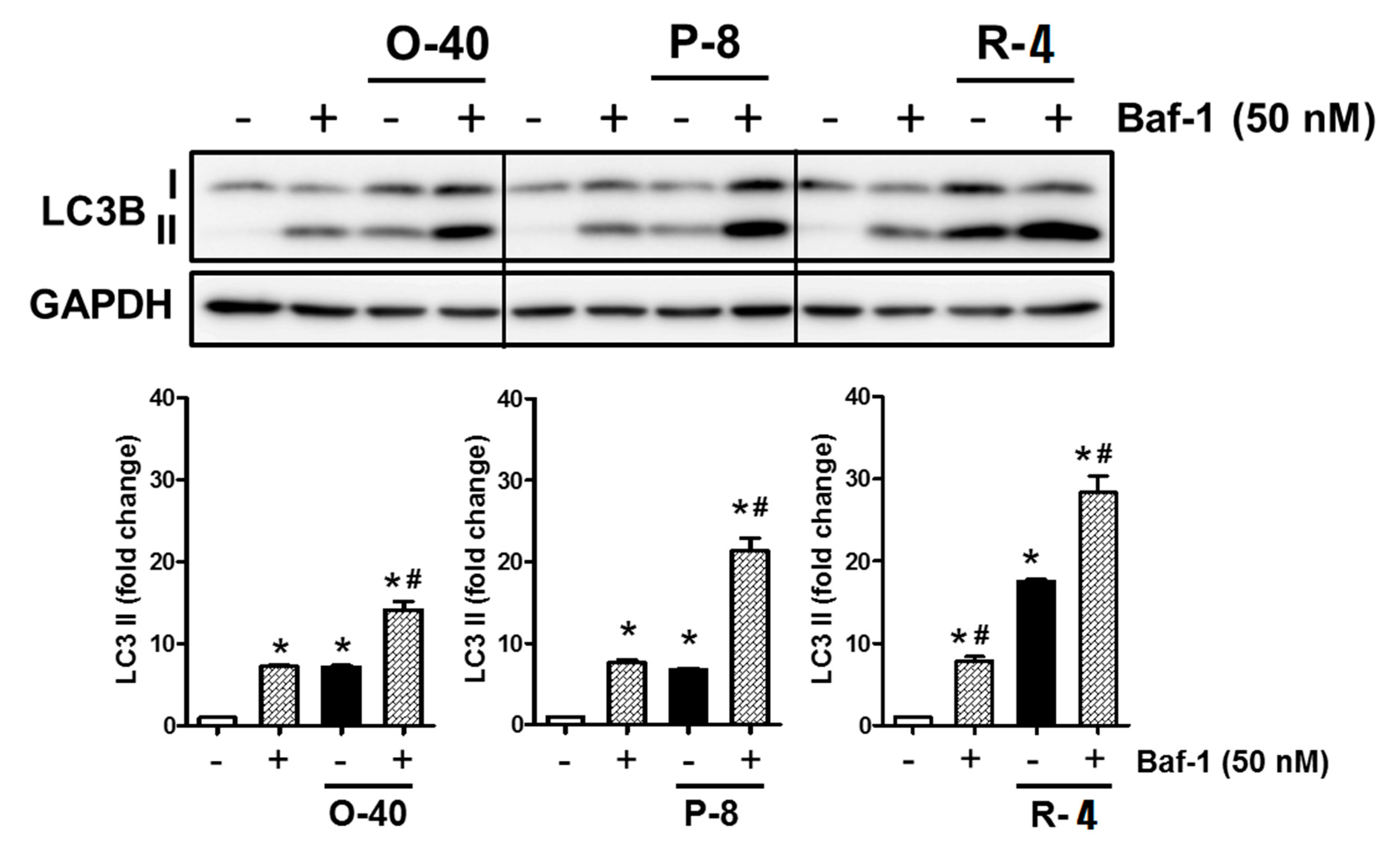
3.7. 5-HT3RAs Act as Autophagy Inducers in A549 Cells
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
Appendix A

References
- Coffey, J.C.; Wang, J.H.; Smith, M.J.; Bouchier-Hayes, D.; Cotter, T.G.; Redmond, H.P. Excisional surgery for cancer cure: Therapy at a cost. Lancet Oncol. 2003, 4, 760–768. [Google Scholar] [CrossRef]
- Sugarbaker, E.V.; Ketcham, A.S. Mechanisms and prevention of cancer dissemination: An overview. Semin. Oncol. 1977, 4, 19–32. [Google Scholar] [PubMed]
- Fortner, J.G. Inadvertent spread of cancer at surgery. J. Surg. Oncol. 1993, 53, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Morgan, T.M.; Lange, P.H.; Porter, M.P.; Lin, D.W.; Ellis, W.J.; Gallaher, I.S.; Vessella, R.L. Disseminated tumor cells in prostate cancer patients after radical prostatectomy and without evidence of disease predicts biochemical recurrence. Clin. Cancer Res. 2009, 15, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.; Le Marer, N.; Wharton, R.Q.; Khan, Z.A.; Araia, R.; Glover, C.; Henry, M.M.; Allen-Mersh, T.G. Clearance of circulating tumor cells after excision of primary colorectal cancer. Ann. Surg. 2002, 235, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Uen, Y.-H.; Lu, C.-Y.; Tsai, H.-L.; Yu, F.-J.; Huang, M.-Y.; Cheng, T.-L.; Lin, S.-R.; Wang, J.-Y. Persistent presence of postoperative circulating tumor cells is a poor prognostic factor for patients with stage I–III colorectal cancer after curative resection. Ann. Surg. Oncol. 2008, 15, 2120. [Google Scholar] [CrossRef]
- Janni, W.; Vogl, F.D.; Wiedswang, G.; Synnestvedt, M.; Fehm, T.N.; Jückstock, J.; Rack, B.; Borgen, E.; Braun, S.; Solomayer, E. Persistence of disseminated tumor cells in the bone marrow of breast cancer patients predicts increased risk for relapse—A European pooled analysis. Clin. Cancer Res. 2011, 17, 2967–2976. [Google Scholar] [CrossRef] [PubMed]
- Knutson, K.L.; Disis, M.L. Tumor antigen-specific T helper cells in cancer immunity and immunotherapy. Cancer Immunol. Immunother. 2005, 54, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Zamarron, B.F.; Chen, W. Dual roles of immune cells and their factors in cancer development and progression. Int. J. Biol. Sci. 2011, 7, 651–658. [Google Scholar] [CrossRef]
- Neeman, E.; Ben-Eliyahu, S. Surgery and stress promote cancer metastasis: New outlooks on perioperative mediating mechanisms and immune involvement. Brain Behav. Immun. 2013, 30, S32–S40. [Google Scholar] [CrossRef]
- Horowitz, M.; Neeman, E.; Sharon, E.; Ben-Eliyahu, S. Exploiting the critical perioperative period to improve long-term cancer outcomes. Nat. Rev. Clin. Oncol. 2015, 12, 213–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenlee, R.T.; Hill-Harmon, M.B.; Murray, T.; Thun, M. Cancer statistics, 2001. CA Cancer J. Clin. 2001, 51, 15–36. [Google Scholar] [CrossRef]
- Asamura, H.; Goya, T.; Koshiishi, Y.; Sohara, Y.; Eguchi, K.; Mori, M.; Nakanishi, Y.; Tsuchiya, R.; Shimokata, K.; Inoue, H. A Japanese Lung Cancer Registry study: Prognosis of 13,010 resected lung cancers. J. Thorac. Oncol. 2008, 3, 46–52. [Google Scholar] [CrossRef] [PubMed]
- King, F.D.; Jones, B.J.; Sanger, G.J. 5-Hydroxytryptamine-3 Receptor Antagonists; CRC Press: Boca Raton, FL, USA, 1993. [Google Scholar]
- Dizeyi, N.; Bjartell, A.; Nilsson, E.; Hansson, J.; Gadaleanu, V.; Cross, N.; Abrahamsson, P.A. Expression of serotonin receptors and role of serotonin in human prostate cancer tissue and cell lines. Prostate 2004, 59, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Sonier, B.; Arseneault, M.; Lavigne, C.; Ouellette, R.J.; Vaillancourt, C. The 5-HT2A serotoninergic receptor is expressed in the MCF-7 human breast cancer cell line and reveals a mitogenic effect of serotonin. Biochem. Biophys. Res. Commun. 2006, 343, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Fanburg, B.L.; Lee, S.-L. A new role for an old molecule: Serotonin as a mitogen. Am. J. Physiol. Lung Cell. Mol. Physiol. 1997, 272, L795–L806. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, E.J.; Shabbir, M.A.; Mikhailidis, D.P.; Mumtaz, F.H.; Thompson, C.S. The effect of serotonin and serotonin antagonists on bladder cancer cell proliferation. BJU Int. 2006, 97, 634–639. [Google Scholar] [CrossRef]
- Cattaneo, M.G.; Palazzi, E.; Bondiolotti, G.; Vicentini, L.M. 5-HT1D receptor type is involved in stimulation of cell proliferation by serotonin in human small cell lung carcinoma. Eur. J. Pharmacol. 1994, 268, 425–430. [Google Scholar] [CrossRef]
- Hoyer, D.; Clarke, D.E.; Fozard, J.R.; Hartig, P.R.; Martin, G.R.; Mylecharane, E.J.; Saxena, P.R.; Humphrey, P.P. International Union of Pharmacology classification of receptors for 5-hydroxytryptamine (Serotonin). Pharmacol. Rev. 1994, 46, 157–203. [Google Scholar]
- Rabasseda, X. Ramosetron, a 5-HT3 receptor antagonist for the control of nausea and vomiting. Drugs Today (Barc.) 2002, 38, 75–89. [Google Scholar] [CrossRef]
- Muchatuta, N.A.; Paech, M.J. Management of postoperative nausea and vomiting: Focus on palonosetron. Ther. Clin. Risk Manag. 2009, 5, 21–34. [Google Scholar] [PubMed]
- Popovic, M.; Warr, D.G.; Deangelis, C.; Tsao, M.; Chan, K.K.; Poon, M.; Yip, C.; Pulenzas, N.; Lam, H.; Zhang, L.; et al. Efficacy and safety of palonosetron for the prophylaxis of chemotherapy-induced nausea and vomiting (CINV): A systematic review and meta-analysis of randomized controlled trials. Support. Care Cancer 2014, 22, 1685–1697. [Google Scholar] [CrossRef] [PubMed]
- Ahn, E.; Choi, G.; Kang, H.; Baek, C.; Jung, Y.; Woo, Y.; Lee, S.; Chang, Y. Palonosetron and Ramosetron Compared for Effectiveness in Preventing Postoperative Nausea and Vomiting: A Systematic Review and Meta-Analysis. PloS ONE 2016, 11, e0168509. [Google Scholar] [CrossRef] [PubMed]
- Lemon, L.S.; Zhang, H.; Hebert, M.F.; Hankins, G.D.; Haas, D.M.; Caritis, S.N.; Venkataramanan, R. Ondansetron Exposure Changes in a Pregnant Woman. Pharmacotherapy 2016, 36, e139–e141. [Google Scholar] [CrossRef] [PubMed]
- Shim, H.-J.; Cho, S.-H.; Chung, I.-J.; Hwang, J.-E.; Bae, W.K.; Kang, G.; Oh, I.-J.; Jung, S.-I. Pharmacokinetic and pharmacodynamic study of ramosetron to prevent chemotherapy-induced nausea and vomiting. J. Clin. Oncol. 2014, 32, e20650. [Google Scholar] [CrossRef]
- Stoltz, R.; Cyong, J.-C.; Shah, A.; Parisi, S. Pharmacokinetic and Safety Evaluation of Palonosetron, a 5-Hydroxytryptamine-3 Receptor Antagonist, in U.S. and Japanese Healthy Subjects. J. Clin. Pharmacol. 2004, 44, 520–531. [Google Scholar] [CrossRef]
- Sarrouilhe, D.; Clarhaut, J.; Defamie, N.; Mesnil, M. Serotonin and cancer: What is the link? Curr. Mol. Med. 2015, 15, 62–77. [Google Scholar] [CrossRef]
- Xu, D.; He, X.; Chang, Y.; Xu, C.; Jiang, X.; Sun, S.; Lin, J. Inhibition of miR-96 expression reduces cell proliferation and clonogenicity of HepG2 hepatoma cells. Oncol. Rep. 2013, 29, 653–661. [Google Scholar] [CrossRef]
- Subramaniam, V.; Ace, O.; Prud’homme, G.J.; Jothy, S. Tranilast treatment decreases cell growth, migration and inhibits colony formation of human breast cancer cells. Exp. Mol. Pathol. 2011, 90, 116–122. [Google Scholar] [CrossRef]
- Klionsky, D.J. Autophagy: From phenomenology to molecular understanding in less than a decade. Nat. Rev. Mol. Cell Biol. 2007, 8, 931–937. [Google Scholar] [CrossRef]
- Galluzzi, L.; Vitale, I.; Abrams, J.M.; Alnemri, E.S.; Baehrecke, E.H.; Blagosklonny, M.V.; Dawson, T.M.; Dawson, V.L.; El-Deiry, W.S.; Fulda, S.; et al. Molecular definitions of cell death subroutines: Recommendations of the Nomenclature Committee on Cell Death 2012. Cell Death Differ. 2012, 19, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Yonekawa, T.; Thorburn, A. Autophagy and cell death. Essays Biochem. 2013, 55, 105–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denton, D.; Nicolson, S.; Kumar, S. Cell death by autophagy: Facts and apparent artefacts. Cell Death Differ. 2012, 19, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Colecchia, D.; Strambi, A.; Sanzone, S.; Iavarone, C.; Rossi, M.; Dall’Armi, C.; Piccioni, F.; Verrotti di Pianella, A.; Chiariello, M. MAPK15/ERK8 stimulates autophagy by interacting with LC3 and GABARAP proteins. Autophagy 2012, 8, 1724–1740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Lopez, N.; Athonvarangkul, D.; Mishall, P.; Sahu, S.; Singh, R. Autophagy proteins regulate ERK phosphorylation. Nat. Commun. 2013, 4, 2799. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Lopez, N.; Singh, R. ATGs: Scaffolds for MAPK/ERK signaling. Autophagy 2014, 10, 535–537. [Google Scholar] [CrossRef] [PubMed]
- Vinod, V.; Padmakrishnan, C.; Vijayan, B.; Gopala, S.J.P.r. ‘How can I halt thee?’The puzzles involved in autophagic inhibition. Pharmacol. Res. 2014, 82, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Soll, C.; Jang, J.H.; Riener, M.O.; Moritz, W.; Wild, P.J.; Graf, R.; Clavien, P.A. Serotonin promotes tumor growth in human hepatocellular cancer. Hepatology 2010, 51, 1244–1254. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, E.J.; Shabbir, M.; Mikhailidis, D.P.; Thompson, C.S.; Mumtaz, F.H. The role of serotonin (5-hydroxytryptamine1A and 1B) receptors in prostate cancer cell proliferation. J. Urol. 2006, 176, 1648–1653. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Population | Propensity-Matched Population | |||||
|---|---|---|---|---|---|---|
| P-R Group (n = 308) | No P-R Group (n = 98) | p-Value | P-R Group (n = 120) | No P-R Group (n = 60) | p-Value | |
| Age | 68.7 ± 9.7 | 67.0 ± 10.7 | 0.144 | 67.9 ± 9.8 | 68.4 ± 9.7 | 0.718 |
| Sex (M/F) | 239/69 | 77/21 | 0.840 | 85/35 | 44/16 | 0.810 |
| BMI | 23.60 ± 2.84 | 22.93 ± 3.82 | 0.113 | 23.73 ± 3.05 | 23.18 ± 2.99 | 0.2535 |
| Comorbidity | ||||||
| HTN | 92 (29.87) | 35 (35.71) | 0.286 | 34 (28.33) | 21 (35) | 0.427 |
| DM | 43 (13.96) | 12 (12.24) | 0.666 | 18 (15) | 7 (11.67) | 0.377 |
| Cancer stage | <0.0001 | 0.855 | ||||
| I | 228 (74.03) | 49 (50) | 93 (77.50) | 46 (76.67) | ||
| II | 39 (12.66) | 31 (31.63) | 19 (15.83) | 10 (16.67) | ||
| III | 38 (12.34) | 18 (18.36) | 8 (6.67) | 4 (6.67) | ||
| Pathology | 0.1278 | 0.801 | ||||
| Squamous cell carcinoma | 67 (21.75) | 30 (30.61) | 31 (25.83) | 14 (23.34) | ||
| Adenocarcinoma | 222 (72.08) | 65 (66.33) | 84 (70) | 44 (73.34) | ||
| Others | 19 (6.17) | 3 (3.06) | 5 (4.17) | 2 (3.34) | ||
| Pre-operative CTx | 19 (6.17) | 9 (9.18) | 0.305 | 9 (7.50) | 4 (6.67) | >0.9999 |
| Operative (op) time | 179.5 ± 73.3 | 183.1 ± 77.8 | 0.702 | 172.3 ± 71.1 | 185.3 ± 76.2 | 0.313 |
| Post-op CTx | 65 (21.10) | 30 (30.61) | 0.053 | 19 (15.83) | 18 (30) | 0.077 |
| Post-op RTx | 5 (1.62) | 2 (2.04) | 0.782 | 2 (1.67) | 1 (1.67) | >0.9999 |
| Recurrence | 76 (24.68) | 44 (44.90) | <0.0001 | 26 (21.67) | 22 (36.67) | 0.005 |
| Mortality | 64 (20.78) | 35 (35.71) | 0.003 | 17 (14.17) | 14 (23.34) | 0.004 |
| Recurrence | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| 5-HT3RA usage | ||||
| No P-R group | 1 | 1 | ||
| P-R group | 0.584 (0.331–1.03) | 0.0634 | 0.547 (0.308–0.974) | 0.0404 |
| Age | 0.987 (0.959–1.015) | 0.3682 | 0.981 (0.954–1.009) | 0.1823 |
| Sex | ||||
| Male | 1 | |||
| Female | 1.285 (0.705–2.342) | 0.4127 | 1.488 (0.793–2.792) | 0.2161 |
| BMI | 1.000 (0.91–1.099) | >0.9999 | ||
| Cancer stage | ||||
| I | 1 | 1 | ||
| II | 2.534 (1.312–4.895) | 0.0056 | 2.641 (1.357–5.137) | 0.0042 |
| III | 3.836 (1.671–8.805) | 0.0015 | 4.451 (1.887–10.498) | 0.0006 |
| Pre-operative HTN | ||||
| No | 1 | |||
| Yes | 0.721 (0.374–1.389) | 0.3279 | ||
| Pre-operative DM | ||||
| No | 1 | |||
| Yes | 1.057 (0.474–2.357) | 0.8918 | ||
| Pre-operative CTx | ||||
| No | 1 | |||
| Yes | 0.78 (0.242–2.513) | 0.6777 | ||
| Operative time | 0.996 (0.992–1.001) | 0.0823 | ||
| Post-operative CTx | ||||
| No | 1 | |||
| Yes | 0.779 (0.377–1.61) | 0.5001 | ||
| Post-operative RTx | ||||
| No | 1 | |||
| Yes | 0 | 0.9841 | ||
| Pathology | ||||
| Squamous cell carcinoma | 1 | |||
| Adenocarcinoma | 1.272 (0.613–2.636) | 0.5182 | ||
| Others | 1.626 (0.351–7.525) | 0.5342 | ||
| Expire | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| 5-HT3RA usage | ||||
| No P-R group | 1 | 1 | ||
| P-R group | 0.611 (00.301–1.241) | 0.1729 | 0.553 (0.264–1.158) | 0.1164 |
| Cancer stage | ||||
| I | 1 | 1 | ||
| II | 2.421 (1.045–5.612) | 0.0392 | 2.085 (0.846–5.139) | 0.1106 |
| III | 4.5 (1.771–11.436) | 0.0016 | 5.872 (2.179–15.82) | 0.0005 |
| Sex | ||||
| Male | 1 | |||
| Female | 1.391 (0.666–2.903) | 0.3794 | 1.854 (0.842–4.081) | 0.125 |
| Age | 0.986 (0.951–1.022) | 0.4381 | 0.974 (0.941–1.009) | 0.1402 |
| BMI | 1.008 (0.897–1.133) | 0.8931 | ||
| Pre-operative HTN | ||||
| No | 1 | |||
| Yes | 0.398 (0.153–1.037) | 0.0594 | ||
| Pre-operative DM | ||||
| No | 1 | |||
| Yes | 0.628 (0.191–2.065) | 0.4434 | ||
| Operative time | 0.996 (0.99–1.001) | 0.0986 | ||
| Pre-op CTx | ||||
| No | 1 | |||
| Yes | 0.373 (0.051–2.733) | 0.3317 | ||
| Post-op CTx | ||||
| No | 1 | |||
| Yes | 0.517 (0.181–1.478) | 0.2184 | ||
| Post-op RTx | ||||
| No | 1 | |||
| Yes | 0 | 0.988 | ||
| Pathology | ||||
| Small cell carcinoma | 1 | 1 | ||
| Adenocarcinoma | 0.466 (0.218–0.995) | 0.0486 | 0.520 (0.230–1.175) | 0.1159 |
| Others | 2.097 (0.584–7.521) | 0.256 | 3.565 (0.866–14.681) | 0.0784 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.S.; Park, S.Y.; Kim, N.Y.; Kim, D.W.; Oh, J.E.; Heo, E.; Lee, J.S.; Yoo, Y.C. Anti-Tumor Potential of a 5-HT3 Receptor Antagonist as a Novel Autophagy Inducer in Lung Cancer: A Retrospective Clinical Study with In Vitro Confirmation. J. Clin. Med. 2019, 8, 1380. https://doi.org/10.3390/jcm8091380
Lee JS, Park SY, Kim NY, Kim DW, Oh JE, Heo E, Lee JS, Yoo YC. Anti-Tumor Potential of a 5-HT3 Receptor Antagonist as a Novel Autophagy Inducer in Lung Cancer: A Retrospective Clinical Study with In Vitro Confirmation. Journal of Clinical Medicine. 2019; 8(9):1380. https://doi.org/10.3390/jcm8091380
Chicago/Turabian StyleLee, Jeong Soo, Seong Yong Park, Na Young Kim, Dong Wook Kim, Ju Eun Oh, Eunjin Heo, Jong Seok Lee, and Young Chul Yoo. 2019. "Anti-Tumor Potential of a 5-HT3 Receptor Antagonist as a Novel Autophagy Inducer in Lung Cancer: A Retrospective Clinical Study with In Vitro Confirmation" Journal of Clinical Medicine 8, no. 9: 1380. https://doi.org/10.3390/jcm8091380